There are different potential risks to shoulder dystocia. Most of these risks are avoidable if the care provider and birth team supporting the birth is trained and skilled it assisting the baby in maneuvering the birth canal quickly and without injury. The following are some of the potential risks.
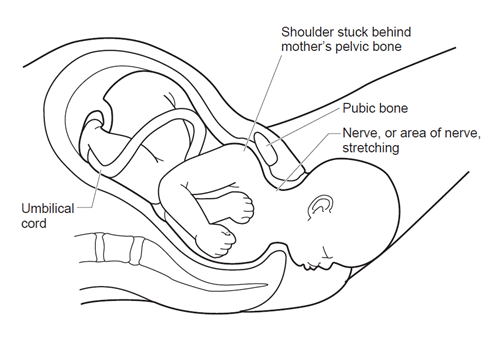
If a baby’s head continues to descend in the birth canal but the shoulder is caught behind the pubis symphysis or sacral promontory of the pelvis, it can stretch or tear the brachial plexus nerves. This damage can be irreversible and impair the motor function of the baby’s arm. This same damage can occur if the care provider attending the birth attempts to pull or twist the baby’s head out before releasing the shoulder from behind the pelvis.
The majority of of cases of shoulder dystocia occur in those without risk factors. Care providers should always be on the lookout for signs of shoulder dystocia and be prepared to move quickly in the event it occurs. This is because while dystocia is statistically more likely to occur on a larger baby, that isn’t a hard rule and providers do not always know if a baby is going to be big or not.
I have had several client’s providers voice concern and counsel the family about a baby being potentially large after an ultrasound because the increased risk of shoulder dystocia. Yet, ultrasound is an incredibly unreliable way to diagnose a ‘big baby’. Using ultrasound to diagnose big baby only has an accuracy rate of 22-37%. Although 1 out of 3 U.S. women are told they have a big baby at the end of pregnancy, only 1 in 10 babies is actually born big (Evidence Based Birth).
A ‘big baby’ or macrosomic baby can be any baby who weighs over 4,500g or 9.9bs. But care providers have not actually made a hard definition of what a macrosomic baby weighs.
A provider will try to find out if a baby is going to be large or not by using ultrasound. Unfortunately, using ultrasounds to predict a baby’s weight is very unreliable. Sonography is only 22-69% accurate at predicting a macrosomnic baby. Yet, providers will often urge parents to undergo unnecessary cesarean sections to prevent a shoulder dystocia and the babies are most often a completely average size and weight. Unfortunately, “it would take nearly 3,700 unnecessary Cesareans to prevent one case of permanent injury due to shoulder dystocia in a baby that is suspected of weighing 9 lbs., 15 oz. or greater.” (Evidence Based Birth).
Shoulder dystocia occurs 5-7% for babies who weigh over 4,000g or 8.8lbs. Yet, Half of all instances of shoulder dystocia occur in babies weighing less than 4,000g (about 9 lb). (RCOG)
Babies who are born to parents who have gestational diabetes are 2-6x more likely to have a shoulder dystocia during their birth. This isn’t just because they have a higher rate of macrosomnia, but because gestational diabetes babies are more likely to have proportionally wider shoulders than non-gestational diabetes babies.
However, pregnant people who manage their gestational diabetes through diet, exercise, or medication can bring down their chances of having a big baby to normal levels (or about 7%) (Landon et al. 2009).

Jenni Jenkins – Sekine is an Oklahoma City Bereavement, Birth, & Postpartum doula and Child Birth Educator who serves her Central Oklahoma community. She is also a midwifery assistant with Holistic Birthing Services and began her journey as a student midwife with the Midwives College of Utah in 2022.
Jenni is also the creator & facilitator of the Kaleidoscope OKC LGBTQ Family Support Group & the Nurture Oklahoma Live Interview Series.
To learn more about Jenni, please click here.