What is Shoulder Dystocia?
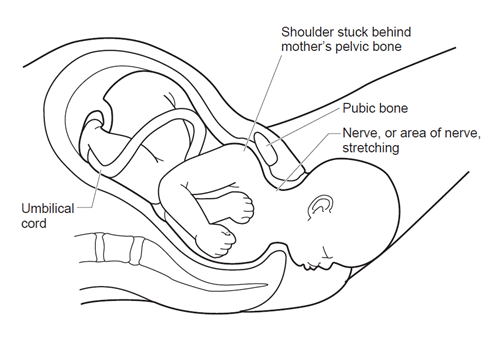
Shoulder dystocia is defined as “failure of the shoulders to spontaneously negotiate the pelvis after delivery of the fetal head, requiring additional obstetric maneuvers beyond gentle downward traction to achieve delivery (ACOG, 2002). More simply, it is when the shoulder of a baby who is being born vaginally gets their shoulder ‘stuck’ behind their parents pelvis.
This isn’t a tissue or skin problem that can solved with ripping or cutting the perineal tissue (an episiotomy), but a bone on bone problem that all birth team members should be trained and prepared for in the incidence that it happens. This is because it is unpredictable regardless if parents show potential risk factors or not.
What Causes Shoulder Dystocia?
Shoulder dystocia is caused by a baby’s shoulder getting caught behind their parent’s pelvis. The shoulder can become caught because the baby has a large shoulder width or they need assistance maneuvering past the pelvis via positioning or care provider intervention. There are a few suspected risk factors like gestational diabetes, bigger babies, and use of an epidural. Yet, because shoulder dystocia is so unpredictable, it doesn’t have a hard set of reliable risk factors.
What are the Risks of Shoulder Dystocia?
There are several potential risks to a shoulder dystocia occurring and not being handled quickly by a trained care provider or birth team. These potential risks include Brachial Plexus Nerve Damage, postpartum hemorrhage, and newborn complications. To read more about the potential risks and who may be at risk of shoulder dystocia, please click here.
Can Shoulder Dystocia Be Prevented?
Something really interesting about this particular birth emergency is that there is no way to accurately predict a shoulder dystocia. “Shoulder dystocia is an unpredictable and unpreventable obstetric emergency. Studies have shown that prepregnancy, antepartum, and intrapartum risk factors have extremely poor predictive value for shoulder dystocia.” (ACOG, 2017). Because it is unpredictable and happens unexpectedly during the labor and delivery process, care providers and members of the birth team need to be trained and prepared to relieve a shoulder dystocia quickly without causing harm to the parent or baby.
Are Cesarean Section surgeries an appropriate preventative?
Is inducing birth early an appropriate preventative?
Just like using cesarean sections to prevent shoulder dystocia, using potential risk factors are unreliable, and shoulder dystocia cannot be accurately predicted. So, inducing to prevent potential shoulder dystocia when you can’t accurately predict who will even have dystocia is not evidence-based.
Let’s not forget that the induction of labor has several of its own risks for maternal and neonatal outcomes. Inducing labor increases your chances of cesarean section, has increased chances of postpartum hemorrhage, increases risks of infection, possible uterine rupture, and more.
Even still, most of the families whose care providers talked about induction for big babies ended up being medically induced (67%) (Evidence-Based Birth). Some care providers do not offer families a choice regarding inducing labor for a suspected big baby to prevent dystocia! “Nearly one in five survey respondents said they were not offered a choice when it came to induction—in other words, they were told that they must be induced for their suspected big baby” (Evidence Based Birth). Inducing a suspected big baby to prevent dystocia is the fourth most common reason for an induction (making up 16% of all inductions).
How is Shoulder Dystocia solved?
One of the most important things that can be done to prevent injury from a shoulder dystocia is having trained care providers and birth teams who are prepared to release a shoulder at every single birth they attend. Care providers and birth teams can do this using several different techniques. “Several techniques to facilitate delivery exist, and there is evidence that a systematic approach and simulation training can improve outcomes.” (ACOG, 2017).
Here is a fantastic video to show a visual on what shoulder dystocia looks like inside the body and how birth team personnel can release a shoulder dystocia!
The McRoberts Maneuver with Suprapubic Pressure
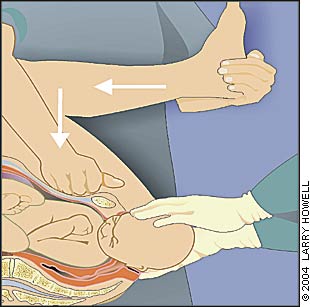
The McRoberts maneuver is when at least two capable, trained birth team personnel aid in the maneuver to push the parent’s legs back towards the parent’s head which hyperflexes the hips and knees. This creates more space for the baby to release their shoulder. This maneuver also helps flatten the sacral promontory or back of the pelvis. Suprapubic Pressure is when a birth team member applies pressure onto the fetal shoulder to push the shoulder both downward (to below the pubic bone) and toward the baby’s face or sternum.
The McRoberts maneuver alone is believed to relieve more than 40 percent of all shoulder dystocias and, when combined with suprapubic pressure, resolves more than 50 percent of shoulder dystocias (American Family Physician).



